Introduction
There are many opportunities for North Carolina lawmakers to help lower the cost of health insurance. One way is to re-examine the 57 health benefit mandates that state officials have passed into law since the 1970s.
Health benefit mandates are laws that force insurance companies to cover specific health-care services, ensure access to desired providers, or expand the level of benefits offered to certain employers and people who purchase insurance policies on their own.
Historically, states have exercised most of the regulatory power over the number and scope of mandates. However, federal intervention accelerated in 1996 under the Newborns and Mothers’ Health Protection Act and the Mental Health Parity Act. These laws specified that, if health plans offered hospitalization care, they were required to cover a minimum length of stay for postpartum women. Additionally, if insurance carriers sold plans that included mental health treatment, those benefits could not be less favorable than the plans’ medical and surgical benefits in terms of out-of-pocket spending and scope of network providers. The Mental Health Parity Act was modified in 2008, requiring employers to offer comparable substance abuse services if they choose to provide mental health benefits for employees.
The 2010 passage of the Affordable Care Act (ACA), commonly known as Obamacare, further extended the federal government’s authority over the insurance industry by enforcing limits on out-of-pocket cost-sharing for policyholders who access certain treatments that fall under the law’s 10 categories of Essential Health Benefits. Required services range from maternity and newborn care to chronic-disease management. The ACA further outlines that policyholders in the individual and group markets can access a variety of preventive services with zero out-of-pocket cost-sharing (see chart below).
Aside from these federal mandates, ample opportunities remain for state legislators to loosen insurance requirements and provide more affordable insurance options for North Carolinians.
Key Facts
- One study concluded that state health insurance mandates were responsible for between 9% and 23% of all premium increases between 1996 and 2011 and affected smaller firms more than larger firms.
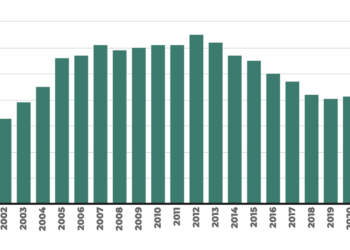
- The insignificant cost of each mandate makes legislation relatively easy to sell to lawmakers. For example, people pay just 5 cents per month for pastoral counseling services. Access to dentists costs $1.02. Seeing a podiatrist amounts to $2.17. This partly explains why there are now 2,200 mandates nationwide, up from almost zero in the 1970s. Individually, each mandate costs little, but collectively, they make insurance policies more expensive.
- Because of the added costs associated with state benefit mandates, small businesses are discouraged from offering health coverage to their employees. A 2021 survey found that one in three small-business owners reported that it was a challenge to obtain health insurance coverage for their employees during the pandemic.
- Not all businesses are subject to state health benefit mandate laws. Self-insured employers are exempt under the 1974 Employment Retirement Income Security Act. Nationwide, 65% of covered workers were enrolled in a self-funded plan in 2022. However, the exemption from state regulation does not deter these firms from offering generous health benefits to their workers.
- Another self-insured, mandate-free entity that provides generous coverage is North Carolina’s State Health Plan. There are cases in which all members of the State Health Plan, including legislators, are subject to health benefit mandates. But there are some exceptions in which legislators exempt the State Health Plan from health mandates they have voted to become law for other plans.
Recommendations
1. Reduce benefit mandates.
Legislators should allow for optimal competition among insurance companies and providers to let them best serve patients and respond to policyholder demands. Consumers should be able to select from insurance options with varying amounts of coverage; insurance plans with less coverage can provide affordable and sensible options, especially for younger, healthier customers who need only basic catastrophic coverage.
2. Determine which health benefit mandates are indeed cost-effective and which ones are used by most policyholders.
More than half the states have mandated benefit review procedures to weigh the cost/benefit factors for any introduced mandate. Others conduct a retrospective analysis of all benefits that have been signed into law.
No Patient Cost-Sharing Allowed Under Affordable Care Act For Preventative Services
Evidence-Based Screenings and Counseling
- Depression
- Diabetes
- Cholesterol
- Obesity
- Cancer
- HIV
- Drug and tobacco use
- Healthy eating
Vaccines
- Influenza
- Tetanus
- Hepatitis A and B
- Measles
Preventative Services: Children and Youth
- Vision impairment
- Autism screening
- Iron and fluoride supplements
- Behavioral and developmental assessments
Preventative Services: Women
- Well-woman visits
- Contraceptives
- Breastfeeding support and supplies
- Domestic violence screening
Source: The Henry J. Kaiser Family Foundation; Preventative Services Covered by Private Health Plans Under the Affordable Care Act
North Carolina Health Benefit Mandates
- Procedures involving the jaw, face, or head
- Anesthesia and hospital charges for dental procedures
- Postmastectomy inpatient care
- Treat maternity as any other illness
- Bone mass measurement
- Prescription drug contraceptives or devices
- Colorectal cancer screening
- Synchronization of prescription refills
- Coverage for emergency care
- Autism Spectrum Disorder
- Services provided outside provider networks
- Mental illness minimum coverage
- Access to nonformulary drugs
- Access to specialist care for managed care plans
- Prescription drugs during an emergency or disaster
- Selection of specialist as a primary care physician
- Selection of pediatrician as primary care physician for minors
- Certain clinical trials
- Newborn hearing screening
- Ovarian cancer surveillance tests
- Diagnosis and treatment of lymphedema
- Hearing aids
- Comply with Public Health Service Act
- Nurse services
- Physician assistant services
- Right to choose providers
- Right to choose chiropractor
- Prohibition on exclusion of claims subject to Workers’ Compensation Act
- Limitations on exclusionary periods for consideration of preexisting conditions
- Coverage for use of intoxicants and narcotics
- Previous creditable coverage for individual health plans
- Eligibility extension for dependents who are mentally or physically handicapped
- Coverage for newborn and foster kids and coverage for congenital defects and anomalies
- Pharmacy of choice
- Direct access to OB/GYN
- Minimum benefit offering for alcoholism/drug abuse treatment
- Mammograms and cervical cancer screening
- Prostate cancer screening
- Certain off label drug use for the treatment of cancer
- Certain treatment of diabetes
- Group replacement requirements
- Coverage for children
- Coverage for adopted children
- Group continuation
- Individual conversion policy
- Limits on the definition of a preexisting condition
- Small employer group guaranteed availability provision
- Guaranteed renewability of employer group health plans
- HIPPA eligible individual guaranteed availability provision
- Complications during pregnancy
- Treatment of HIV/AIDS
- Renewability standard for individual Accident and Health policy