Americans are understandably frustrated when they hear that drug costs in the United States are roughly three times higher than they are in Europe. But President Trump’s executive order requiring that drug companies set their U.S. prices at the lowest price available in other developed countries will damage the market while failing to bring down costs.
The executive order issued last year attempts to create a most-favored-nation prescription drug pricing system, by which drugs would be sold on terms equal to or better than in other countries. Some states have already implemented their own laws with various types of mandates for lower drug prices.
These types of proposals attempt to address an actual problem facing the American health care system. Many of the wealthiest countries in the world are paying lower prices for prescription drugs than the United States thanks to their internal regulatory policies and government control over drug purchases. That shifts costs to Americans and harms all countries by depressing drug development. The United States is one of the few countries contributing to research and development costs.
However, mandating most-favored-nation prescription drug pricing actually makes this problem worse. It does not stop foreign freeloading but contributes to it by basing U.S. prices on the prices in countries that pursue their own agendas for their government-dominated healthcare systems.
The hope of a drug price MFN policy is that it will give manufacturers the incentive to negotiate better deals with European companies, thereby shifting costs from Americans to Europeans. But that is wishful thinking at best. Currently there is little or no negotiation between European governments and manufacturers, forcing U.S. companies into “take-it-or-leave it” propositions. European governments running socialized healthcare systems are monopsony buyers who have all the market power. If American drug companies ever attempted to level the playing field by banding together to negotiate against European governments, the European Commission would prosecute them for collusion in violation of European competition law.
Price controls like the ones in Europe will only create new problems for U.S. patients. Drug shortages are likely to leave some patients without the treatments they need. Another problem is that companies would not be able to recuperate the research and development costs for new medicines they create. That will depress innovation and reduce new drug development for American patients. The United States could soon become a follower, not a leader, in medical innovation.
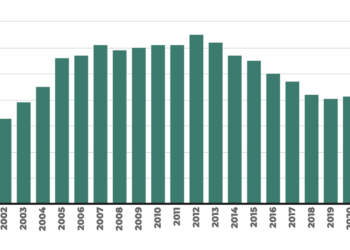
The only country that is well positioned to replace the United States as the leader in medical innovation is China. China’s global share of value-added pharmaceutical output grew from 6% in 2002 to 24% in 2019. China is not turning to price controls as it seeks pharmaceutical dominance, relying instead on subsidies, financial incentives, start-up incubators, public-private partnerships, talent recruitment initiatives, expedited drug reviews, and enhanced IP protection for its own drug innovations.
Chinese emergence as the leading source of pharmaceutical innovation carries great risk. The Covid lockdown in China created a worldwide shortage of iodinated contrast media used for CT scans, causing rationing of diagnostic imaging for almost a year. China’s status as the world’s leading drug innovator gives it more power in trade negotiations and provides leverage it can use to favor other Chinese industries over their American competitors.
American lawmakers have better options. They should instead focus on reforms that unleash the free market, encourage competition and innovation, reduce unnecessary regulatory burdens, and protect intellectual property rights. These policies will be much more effective in lowering drug costs over time while expanding patient choice and preserving incentives for future medical breakthroughs.