Governor Hochul’s focus on affordability seems to have skipped over the healthcare portions of the new state budget.
The deal finalized May 27 between Hochul and the Legislature, which was came almost two months into new fiscal year, allows state Medicaid spending to increase at a double-digit rate while extending what was meant to be a temporary tax on insurance premiums.
The budget’s one major stab at controlling health costs – by reforming an arbitration system for medical billing disputes – applies only to government-operated plans. Private-sector consumers and employers will remain exposed to abusive claims.
Here are the highlights:
Medicaid:
The largest component of the state share of Medicaid spending, known as Department of Health Medicaid, is projected to surge 16.2 percent to $40 billion in fiscal year 2027, according to preliminary figures released by the Budget Division.
As noted by Crain’s New York, that’s $5.6 billion more than the amount for fiscal 2026 and $1.3 billion more than Hochul initially proposed in January.
Officials said this growth is inflated by transactions related to the MCO tax (see below) on Medicaid-funded health plans, in which the state pays half the bill and then collects back that amount plus matching aid from Washington. Without those transactions, the annual growth in DOH Medicaid would be 7.5 percent.
However, that does not include projected Medicaid outlays from other state agencies and local governments as well as federal matching aid, which have not yet been published. Those combined amounts will likely bring the program’s total budget to $120 billion or more. A full accounting from the Budget Division is due late this month.
New York’s version of the safety-net health plan has long been the costliest of any state’s on a per-resident basis, and its growth has accelerated sharply on Hochul’s watch.
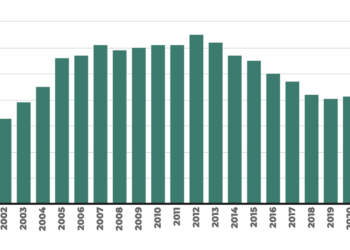
This year’s 16.2 percent increase in DOH Medicaid is the highest since 2012. That was the aftermath of the Great Recession, when Medicaid enrollment was rising and a temporary boost in federal aid was expiring. Today, by contrast, enrollment is declining and federal aid is rising (exaggerated forecasts about budget cuts in Washington notwithstanding).
Recent increases have largely been spent on higher payments for medical providers. A news release from the governor about this year’s budget itemizes billions in additional funding for reimbursement rates, capital grants and other subsidies.
Insiders have said this year’s budget earmarks $100 million to subsidize one of the benefit funds covering members of the healthcare labor union 1199 SEIU. The approved legislation does not explicitly mention that allocation.
In the past, similar subsidies have flowed through programs with vague or misleading names, such the “Advanced Training Initiative” or the “Quality Incentive Vital Access Provider Program,” which the Health Department created using discretionary funds.
MCO tax
State leaders are choosing to extend their two-year-old tax on health insurance plans even though Washington has closed down the regulatory loophole it was originally designed to exploit.
The existing tax on managed care organizations, or MCOs, mostly applies to Medicaid managed care plans as a tactic for extracting extra matching funds from Washington. It produces net revenue of roughly $1.8 billion per year, but it’s contingent on federal approval that’s due to lapse in December.
Rather than cancelling the tax completely, lawmakers are replacing it as of January 2027 with a version that will comply with updated federal regulations.
Whereas the old tax charged widely varying per-person rates and raised most of its revenue from Medicaid plans, the new tax will charge all health plans a flat 0.35 percent of premiums. Based on the average individual premium from 2024, that would amount to about $35 per person. The old MCO tax on commercial plans was $18 to $24 per person.
The modified MCO tax is expected to bring in about $165 million in its first year, according to a memo from the Greater New York Hospital Association, which supported the extension.
The new premium tax layers on top of the state’s existing health insurance taxes that already add between 7 percent and 14 percent to health costs for employers and consumers, according to insurance industry estimates.
It also gives hospitals and other providers a vehicle for seeking more money next year, as GNYHA made clear:
“While the new MCO tax generates significantly less revenue than the current tax, it serves as an important placeholder for future budget negotiations,” the group said in its memo. “We believe that it would be very difficult to resurrect the MCO tax in the future if it were allowed to sunset in December.”
Although annual revenue from the MCO tax is slated to drop more than 98 percent –- from $1.8 billion to $167 million – lawmakers are using the money to finance $1.5 billion in increased funding for hospitals, nursing homes, clinics and other providers in this year’s budget. This sets the stage for a budget crunch in fiscal 2028, when lawmakers will likely face pressure to continue the spending financed by the MCO tax even as the revenue dries up.
Essential Plan
In a surprising development, the budget appropriates a record-high $14.9 billion for the Essential Plan, almost entirely from federal funds. That’s an increase of $1.8 billion or 14 percent from fiscal 2026, even though the program will be shedding 434,000 enrollees as of July.
Officials said the appropriation does not necessarily reflect the state’s projected revenue or spending for the program, which it will be releasing along with the enacted budget financial plan in a few weeks.
However, the amount suggests that the financial hit to the program from last year’s federal budget cuts might be smaller than officials previously estimated.
Last year, the Hochul administration had warned that the program stood to lose $7.5 billion in federal aid. This was because legally present immigrants – which had made up 43 percent of the plan’s enrollment and generated 55 percent of its revenue – were made ineligible as part of last summer’s federal spending bill.
In response to those changes, the state reversed a 2024 expansion of the program. This enabled the state to dip into billions in previously accumulated reserves, but it also displaced some 430,000 enrollees between 200 percent and 250 percent of the poverty level.
Despite the high stakes of its revisions to the Essential Plan, which involved billions in funding and more than 1 million enrollees, the Hochul administration has yet to publish a financial plan delineating those changes.
The program has a history of generating unexpectedly large amounts of federal aid, causing billions of dollars to accumulate in a trust fund. It will be interesting to see if that pattern continues.
Dispute resolution
The final budget gave Hochul a partial victory in her attempt to crack down on abuse of the state’s “no surprises” law for emergency-related health insurance claims.
Medicaid will now be exempt from the law, and the state employee health plan will operate under the tightened rules that Hochul proposed. However, lawmakers rejected changes with respect to the commercial insurance plans used by small and medium-sized employers as well as individual consumers.
Hochul was responding to the rapid growth in the use of “independent dispute resolution,” or IDR, an arbitration system in which out-of-network emergency providers can seek higher payment from insurers. According to statistics from the Department of Financial Services, requests for IDR have soared by more than 1,700 percent in five years – from 2,500 in 2020 to almost 47,000 in 2025.
Many of these cases have challenged payments by Medicaid managed care plans, which the law was not designed to handle.
There has been a similarly sharp increase in utilization of the federal “no surprises” law as certain medical practices effectively have outsourced much of their billing to legal firms that specialize in arbitrating claims.
Under the final budget, lawmakers agreed to exempt Medicaid from IDR and to tighten the rules for disputing claims involving the New York State Health Insurance Plan, which covers government employees.
However, they opted to keep the status quo for commercial insurance plans, which drew an sharp reaction from the New York State Conference of Plans:
“This budget had the potential to lower healthcare costs for every New Yorker,” the conference wrote in a post on X. “Instead, the Governor and the Legislature chose to limit healthcare savings to state-run accounts while leaving the general commercial market at the mercy of inflated provider rates and destabilizing contract disputes. New York families deserve the same healthcare cost protections that the state provides for itself.”