

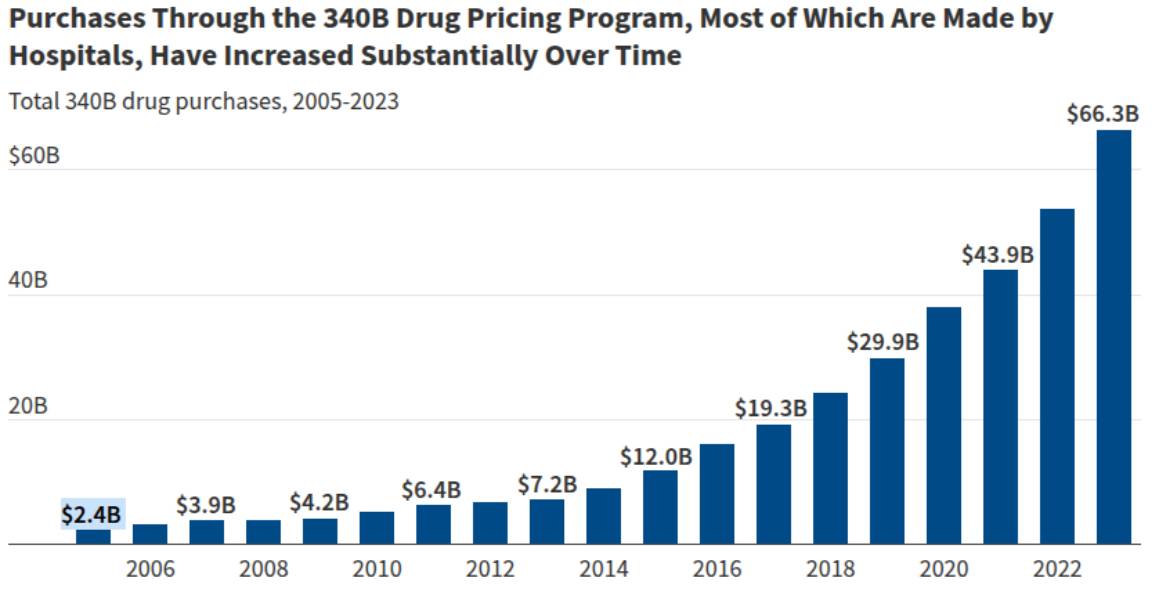
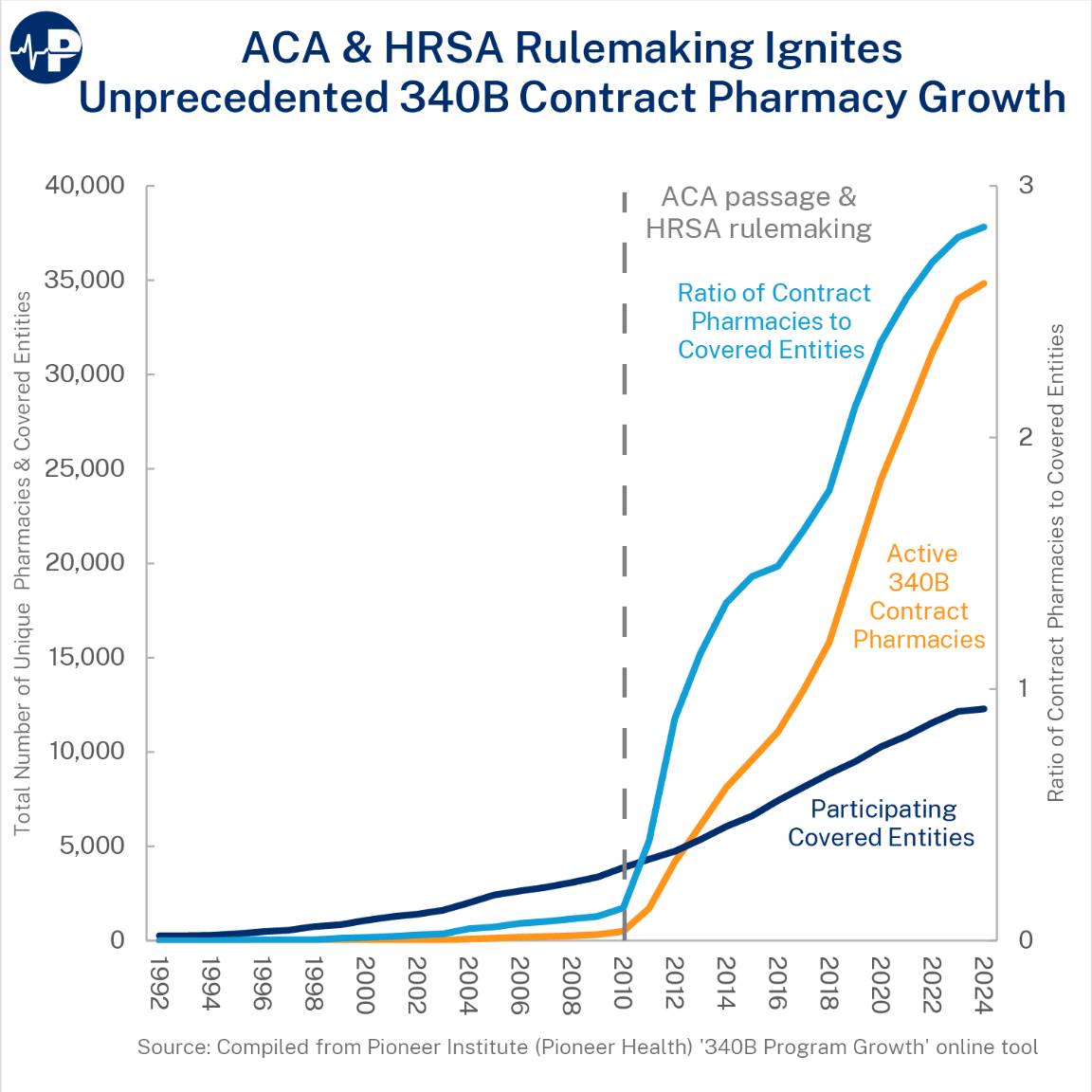
The federal 340B program allows some hospitals and medical clinics to buy drugs from manufacturers at a huge discount and then resell them for large profits. Initially a relatively small program, a rule during the Obama Administration skyrocketed the program’s usage.
This has quickly become an unaccountable slush fund. The law essentially requires drug manufacturers to give money to hospitals and pharmacies, which is not an appropriate use of the federal government’s power. The program was intended to be used by a few hospitals in poor areas serving largely low-income patients. But the Obama-era rule allowed these hospitals to outsource to pharmacies and made it easier to shift the money elsewhere.
There is a campaign by pharmacies, hospitals and other allies to keep this revenue going. A group has started an advertising campaign to urge Michigan lawmakers to protect and expand 340B because it “provides access to affordable healthcare across the state.”

The evidence for this is scant. The hospitals able to use the 340B program get higher profits but provide less charitable care. Some medical facilities use the program to move money from hospitals in low-income communities to those in high-income communities.
About a decade ago, Michigan raised the income limits of those eligible for Medicaid, increasing the number of people covered by taxpayer-provided health services. From 2014 to today, the number of residents on Medicaid increased from about 1.9 million to 2.4 million. This meant that fewer poor people would need charity care, yet 340B program purchases exploded in use.
The 340B program has become a slush fund for some hospital systems. It allows the same drug to be sold for drastically different prices in order for some medical facilities to keep the money. Conservative leaders are calling for needed changes and Michigan lawmakers have options to fix the program. They ought to notice that it’s not serving the public even as its beneficiaries argue for it to continue.













