
In a previous article, I documented how total Medicaid expenditures in North Carolina surged from $18.14 billion in fiscal year (FY) 2021 to $35.77 billion in FY 2025 — a staggering 97.2 percent increase in just four years.
That growth was fueled not only by Medicaid expansion, but by a financing structure that relies heavily on provider taxes to draw down federal matching dollars and recycle funds back to hospitals through state directed payments.
Recent changes enacted under the One Big Beautiful Bill (OBBB) place this financing model directly at risk. If North Carolina’s Medicaid program is to remain viable over the long term, structural reform is no longer optional. What follows are practical policy prescriptions to restore fiscal sustainability and program integrity while protecting the truly vulnerable.
Medicaid funding loop
To understand why the OBBB poses such a serious threat — and why reform is urgent — it is necessary to first examine how North Carolina’s Medicaid financing model works.
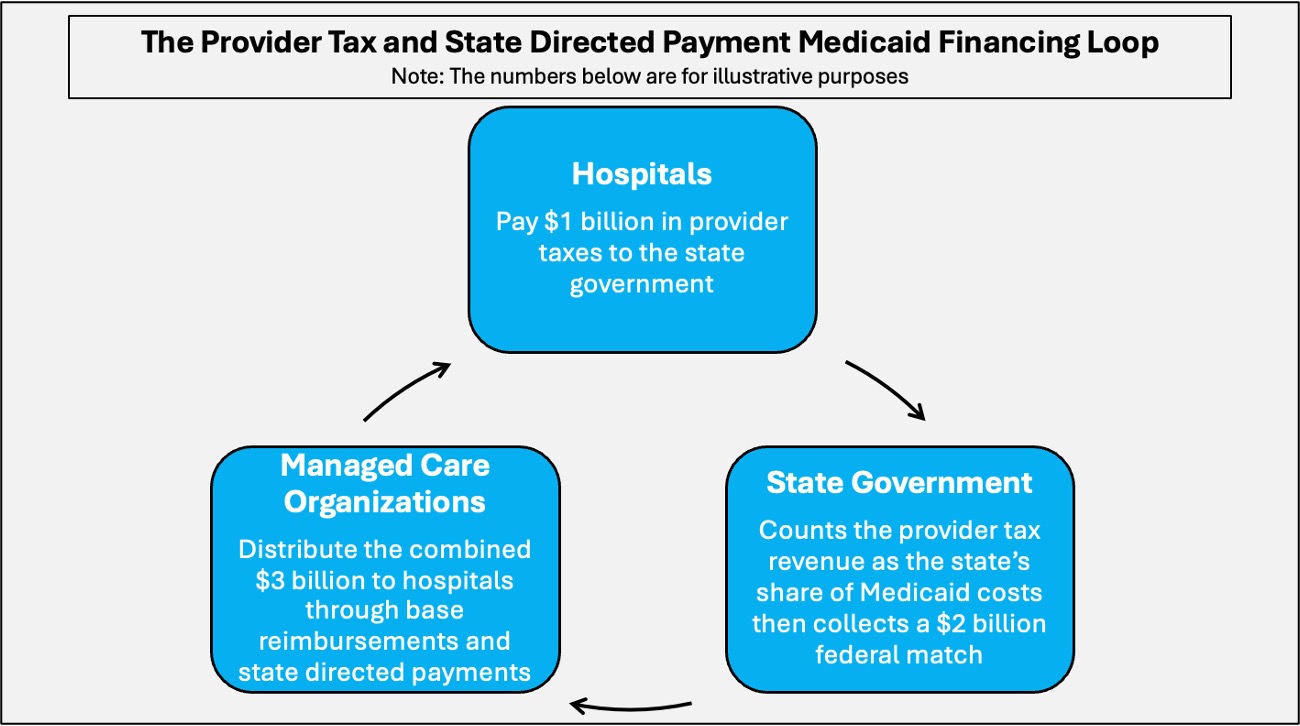
North Carolina relies on a funding loop involving provider taxes and state directed payments that allows the state to leverage federal matching dollars and recycle funds back to hospitals. State directed payments are supplemental payments that states require managed care plans to make to providers to boost reimbursement levels.
Hospitals pay provider taxes to the state, which are used to pay for the state’s share of Medicaid spending. The state then draws down federal matching funds, increasing the total pool of dollars available.
Those combined funds are redistributed to hospitals by managed care organizations through base reimbursements — typically benchmarked to Medicare rates, which provide a nationally standardized reference point — with additional state directed payments layered on top to raise total reimbursement well above Medicare levels.
In practical terms, the more hospitals contribute through provider taxes, the larger the federal match the state can claim, and the greater the total payments ultimately returned to those same hospitals. In fact, North Carolina hiked hospital provider taxes in order to fund Medicaid expansion.
The One Big Beautiful Bill
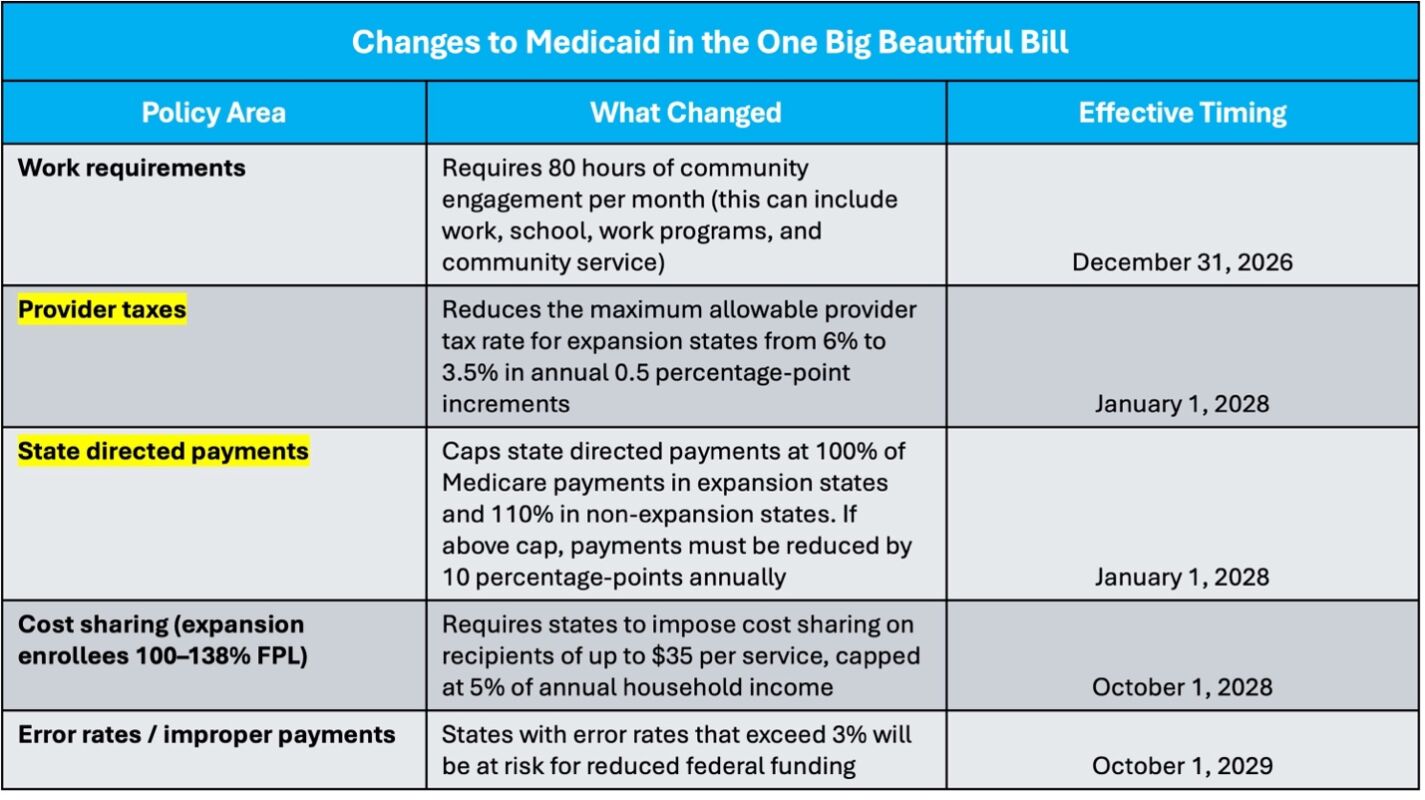
The financing structure outlined above depends on federal rules that are now changing. The OBBB caps state directed payments at Medicare levels in expansion states and phases down allowable provider tax rates from 6 percent to 3.5 percent. Together, these provisions directly constrain the mechanisms North Carolina has relied upon to expand Medicaid spending.
For instance, reducing the provider tax rate would make North Carolina unable to fund its share of expansion population expenses, meaning legislators have just a few years to decide whether they want to allow the expansion population to be kicked off Medicaid, or to find an alternative funding mechanism to keep them in the program.
In addition, the OBBB is implementing an 80-hour-per-month work requirement, cost-sharing for certain expansion enrollees, and a 3 percent limit on improper payment rates for states.
State directed payments
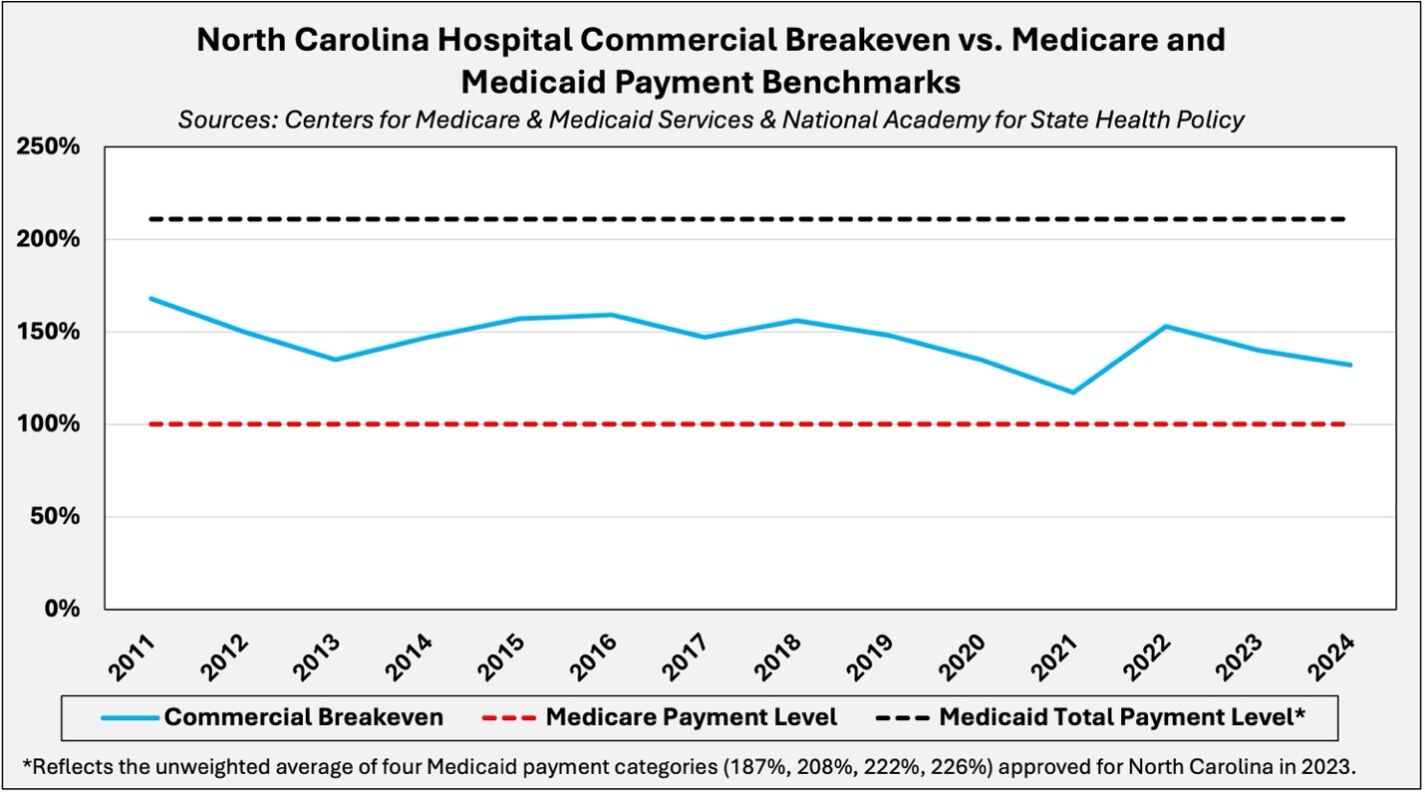
In FY 2023, North Carolina structured its Medicaid financing system to elevate hospital reimbursement far above commercial breakeven levels. As of 2024, the median hospital breakeven rate in North Carolina was approximately 132 percent of the Medicare reimbursement level, yet recent Medicaid payment benchmarks vary from 187 percent to 226 percent of that level.
Under the OBBB, Medicaid reimbursement for expansion states will be capped at 100 percent of the Medicare reimbursement rate. That cap implies a reduction of more than 100 percentage points from North Carolina’s average Medicaid payment level of 211 percent. The reductions are to be implemented in 10 percentage-point increments beginning in 2028.
Policy prescriptions
In light of the federal government unraveling North Carolina’s Medicaid financing structure, the most fiscally responsible long-term reform would be to repeal Medicaid expansion before resorting to other spending cuts, tax increases, or jeopardizing coverage for traditional Medicaid recipients, such as the disabled.
However, if policymakers choose to maintain Medicaid expansion, the following, more targeted reforms should be implemented without delay:
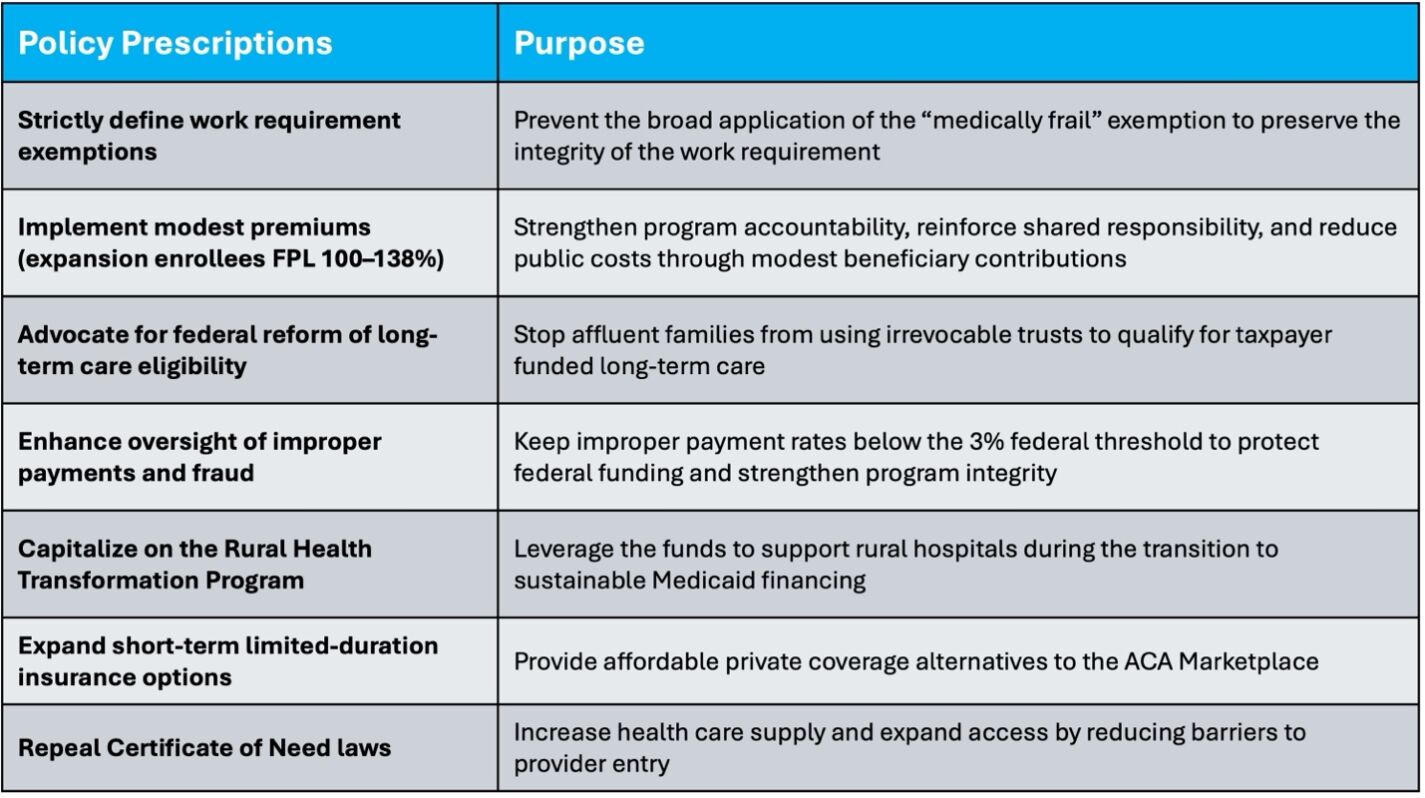
- Strictly define the “medically frail” exemption to prevent abuse and preserve the integrity of the work requirement. The existing exemption categories already encompass a broad range of vulnerable populations.
- Implement modest premiums to reduce certain forms of improper enrollment while slightly easing the burden on taxpayers.
- Advocate for federal reform of long-term care eligibility — particularly asset protection loopholes — which could reduce North Carolina’s Medicaid costs by tens to hundreds of millions annually.
- Strengthen oversight of improper payments to ensure the Medicaid payment error rate does not exceed 3 percent to avoid further reductions in federal funding.
- As part of the OBBB, North Carolina is receiving $213 million from the Rural Health Transformation Program this year, with similar allocations expected for the next four years. Strategically deploying these funds over the next five years can help offset reductions in state directed payments to rural hospitals as the state adjusts its financing structure.
- Short-term limited-duration insurance can provide consumers with an affordable alternative to ACA Marketplace coverage. Expanding these plans from three months to 12 months, with renewals up to 36 months, and allowing consumers to purchase coverage from insurers in US territories would offer lower-cost private options following the expiration of enhanced subsidies last year.
- Finally, repealing the Certificate of Need law would increase health care supply, enhance competition, and help mitigate excessive price pressures.
Closing thoughts
North Carolina’s Medicaid financing model was designed to exploit the federal matching dollars system, but that era is ending.
As the provider tax rate limit declines and the state directed payment cap tightens under the OBBB, the state must transition from relying on federal loopholes to building a sustainable program rooted in fiscal discipline.
The policy prescriptions outlined above are grounded in fiscal reality and structural reform. Together, they can help to restore program integrity, reduce public exposure, and protect the safety net for those it was designed to serve. The clock is ticking, and delaying reform will only make the eventual adjustment more painful.








